Home / Advanced Hemodynamic Monitoring / Cardiac Output (LiDCO)
Cardiac Output (LiDCO)
Monitorización del gasto cardíaco (CO)
Monitorización del gasto cardíaco (CO)
El gasto cardíaco (CO) es la cantidad de sangre que expulsa el corazón por minuto. La monitorización de los componentes del CO permite a los médicos evaluar si hay un volumen suficiente de sangre en el organismo para transportar oxígeno. La monitorización del CO puede ayudar a los médicos a gestionar los fluidos, supervisar las intervenciones terapéuticas y mejorar los resultados de los pacientes.1
La monitorización del CO, junto con otros parámetros hemodinámicos avanzados, está disponible a través del sistema de monitorización hemodinámica Masimo LiDCO®.
Optimización de fluidos
Optimización de fluidos
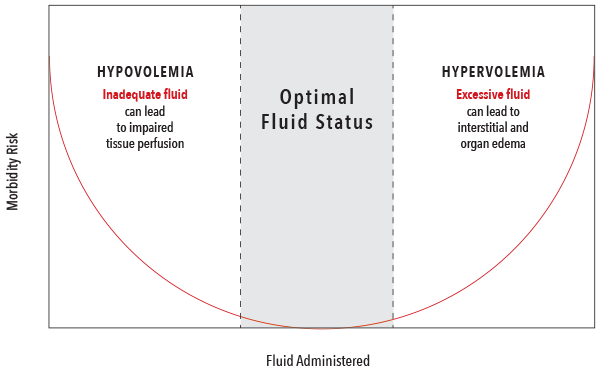
La administración de fluidos es una de las intervenciones más comunes que se realizan para aumentar el CO. Sin embargo, la administración de fluidos debe ser equilibrada para evitar tanto la hipovolemia como la hipervolemia, que se han asociado con resultados negativos.2
Componentes del suministro de oxígeno
Componentes del suministro de oxígeno
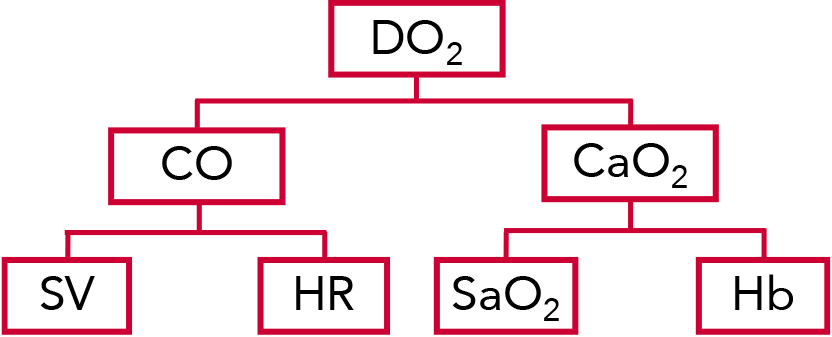
El suministro de oxígeno (DO2) es la cantidad de oxígeno suministrada a los tejidos, que se calcula al multiplicar el CO por el contenido de oxígeno (CaO2).3
El CO se calcula multiplicando el volumen sistólico (SV) por la frecuencia cardíaca (FC) del paciente. El SV es la cantidad de sangre que el ventrículo izquierdo del corazón bombea en una contracción.3
El DO2 y el CaO2 se ven influidos por la saturación de oxígeno (SaO2) y la hemoglobina (Hb) del paciente.3
Parámetros hemodinámicos normales4-8
| Parámetro | Ecuación | Rango normal |
| Suministro de oxígeno (DO2) | CaO2 x CO x 10 | 950-1150 ml/min |
|---|---|---|
| Gasto cardíaco (CO) | FC x SV/1000 | 4,0 – 8,0 l/min |
| Contenido de oxígeno (CaO2) | (1,38 x Hgb x SaO2) + (0,0031 x PaO2) | 17 – 20 ml/dl |
| Volumen sistólico (SV) | N/A | 60 – 100 ml/latido |
| Saturación de oxígeno (SaO2) | N/A | 95 – 100 % |
| Hemoglobina total (Hb) | N/A | Hombres: 13,8-17,2 g/dl Mujeres: 12,1-15,1 g/dl |
| Frecuencia cardíaca (FC) | N/A | El rango varía según el estado del paciente (en reposo o activo, edad, etc.). |
Descripción general de la tecnología del algoritmo PulseCO™
Descripción general de la tecnología del algoritmo PulseCO™
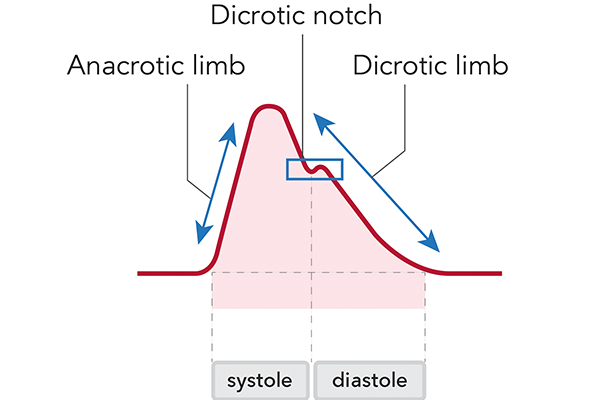
El algoritmo PulseCO™ proporciona CO y SV continuos latido a latido mediante el análisis de una forma de onda de presión arterial. El algoritmo se basa en principios físicos y fisiológicos y se centra en el análisis de la potencia del pulso en lugar de en la forma o el contorno de la onda. A diferencia de otros algoritmos de presión arterial, PulseCO no se basa en estadísticas y suposiciones sobre la distensibilidad vascular, ni en la detección de la muesca dícrota, lo que a menudo supone un reto con las señales arteriales periféricas. Como resultado, el algoritmo PulseCO evita las limitaciones de otras tecnologías de monitorización hemodinámica basadas en la presión del pulso o el contorno.
El estándar de referencia actual en la monitorización hemodinámica, aunque no se utiliza tan comúnmente debido a su carácter invasivo, es el catéter de arteria pulmonar (PAC). El algoritmo PulseCO ha sido validado frente al PAC y ha demostrado una buena concordancia entre ambos métodos.9
Evidencias clínicas de PulseCO
Evidencias clínicas de PulseCO
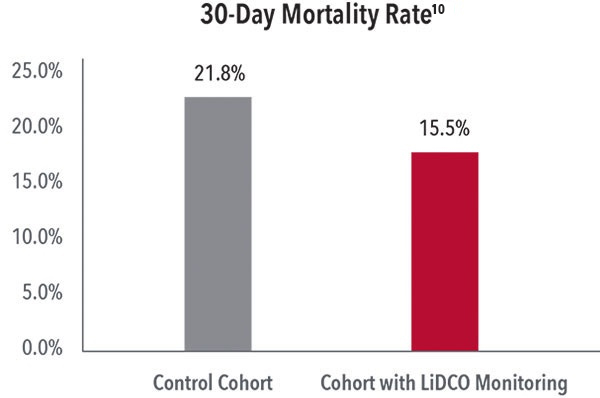
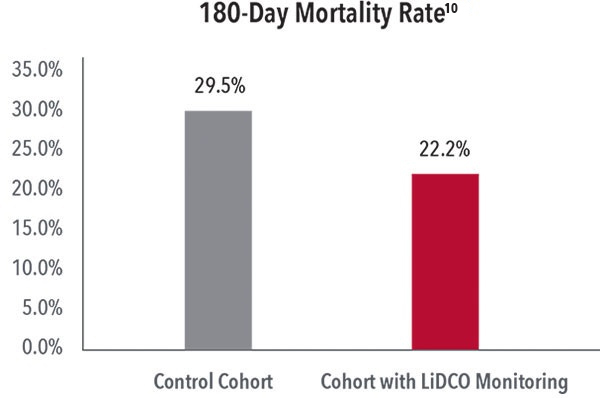
Reducción de la mortalidad a los 30 y 180 días
En un estudio en el que se compararon los resultados de 1200 pacientes sometidos a cirugía abdominal mayor, los investigadores descubrieron que, tras la implementación de un programa que incluía la monitorización LiDCO con tecnología PulseCO, se produjo una disminución significativa de la mortalidad a los 30 días (del 21,8 % al 15,5 %) y a los 180 días (del 29,5 % al 22,2 %).10
Reducción de las complicaciones postoperatorias y los costes
En un ensayo aleatorizado y controlado con 734 pacientes sometidos a cirugía gastrointestinal mayor, los investigadores descubrieron que la optimización hemodinámica con monitorización LiDCO con tecnología PulseCO condujo a una reducción de más del 20 % en las complicaciones postquirúrgicas y, como resultado, el tratamiento de los pacientes monitorizados con monitorización LiDCO con tecnología PulseCO fue, de media, 530 dólares más barato durante 6 meses que el de los pacientes del grupo de control sin monitorización.1, 11
Cartera de productos Masimo LiDCO

Referencias:
- 1.
Pearse R et al. JAMA 2014; 311(21):2181-90.
- 2.
Bellamy MC. Br J Anaesth. Diciembre de 2006; 97(6):755-7.
- 3.
Miller's Anesthesia, 8.ª edición, vol. 2
- 4.
Burns, S. M., & Delgado, S. A. (2019). AACN essentials of critical care nursing (4.ª ed.). Nueva York, NY: McGraw-Hill.
- 5.
Diepenbrock, N. H. (2015). Quick reference to critical care (5.ª ed.). Filadelfia, PA: Wolters Kluwer.
- 6.
Jones, J., & Fix, B. (2015). Critical care notes: Clinical pocket guide (2.ª ed.). Filadelfia, PA: FA Davis.
- 7.
Urden, L. D., Stacy, K. M., & Lough, M. E. (2020). Priorities in critical care nursing (8.ª ed.). San Luis, MO: Elsevier.
- 8.
World Health Organization Global Database on Anaemia. 2008.
- 9.
Costa et al. Intens Care Med. 2007. DOI 10.1007/s00134-007-0878-6 P1.8
- 10.
Tengberg LT et al. Br J Surg 2017; 104:463-471.
- 11.
Sadique Z, et al. Perioper Med (Lond). 14 de diciembre de 2015;4:13.
RECURSOS
Para uso profesional. Consulte las instrucciones de uso para obtener información completa sobre la prescripción, incluidas las indicaciones, contraindicaciones, advertencias y precauciones. Precaución: La legislación federal (EE. UU.) solo permite la venta de este dispositivo a médicos o bajo la prescripción de estos profesionales.
PLCO-008040/PLM-14934B-0126 EN-PLM-13197C